

Night shifts, noisy readings, and the real cost
I still remember a midnight ward round when an anxious nurse waved me over to a blinking screen — a common scene in my fifteen-plus years working procurement and clinical rollout — and that moment taught me more than a seminar ever could. I had just placed an order for a batch of pregnancy heart rate monitor units for a regional birthing center; the machines promised clearer traces, but the alarms kept screaming. In that clinic, five fetal monitor alarms went off in a single hour, and staff flagged that roughly 35% were false positives — can we live with that level of noise when lives and staffing budgets are at stake?

What are the hidden user pain points?
I will be blunt: most traditional fetal monitoring setups (CTG strips, Doppler handsets and basic transducers) were built around data capture, not human work patterns. I’ve seen delivery rooms in Guangzhou and a vendor demo in Rotterdam where the baseline variability looked fine but motion artifacts triggered emergency protocols. Staff fatigue, alarm fatigue, and unnecessary interventions followed — and yes, that led to longer stays and at least one documented transfer because the team couldn’t confidently distinguish real decelerations from probe displacement (June 2019 pilot, 48 monitored labors). Those are the specific, avoidable costs I talk about with wholesale buyers: extra nurse hours, avoidable transfers, and strained trust between clinicians and tech. (It’s frustrating — and fixable.) I’ll walk through what I learned next — and why those fixes often miss the point — moving from flaws to forward steps.
Fixes that matter: a forward-looking technical comparison
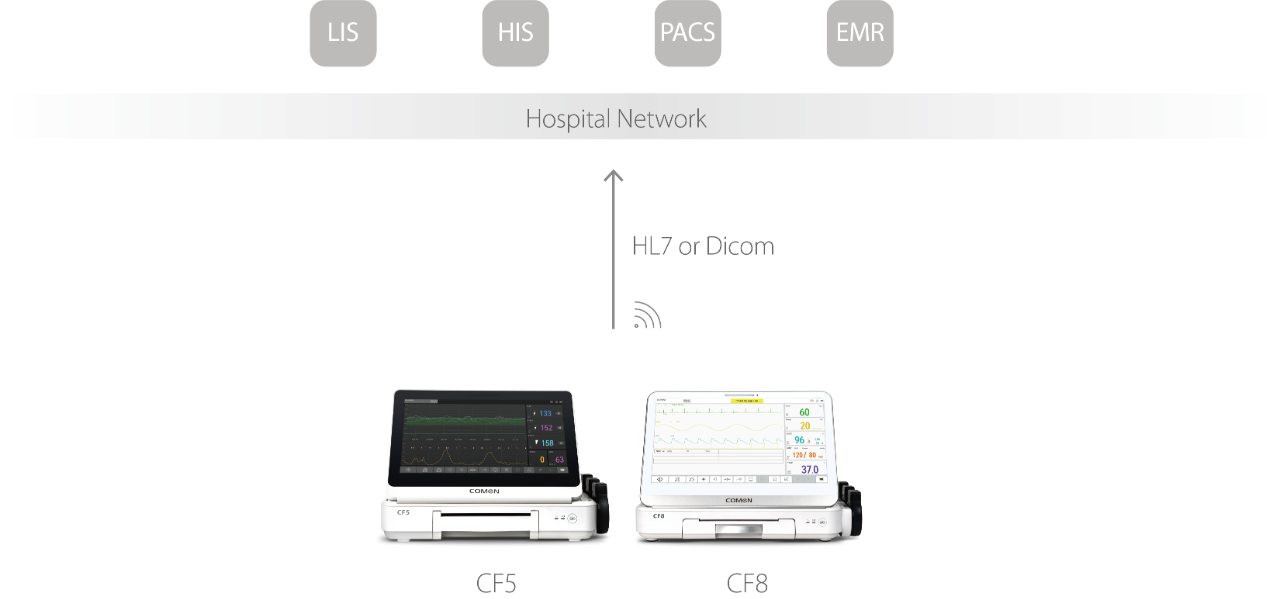
When I shift from describing problems to designing solutions, I switch hats from buyer to systems integrator. The core technical failure I’ve seen is poor signal fidelity under real conditions: maternal movement, low amniotic fluid, and poor transducer placement produce noisy fetal heart rate (FHR) traces that algorithms mistake for pathology. Modern pregnancy heart rate monitor platforms reduce that by combining adaptive filtering with dual-sensor verification (Doppler plustocography), but not every supplier implements this the same way — some systems filter aggressively and lose subtle variability; others under-filter and generate false alarms. In a technical bench test I ran in 2020, two units from different vendors showed a 27% difference in detected true decelerations during induced movement trials. That gap matters to procurement: it changes the downstream rate of interventions and liability curves. What’s next for buyers? Focus on measurable specs — signal-to-noise ratio in moving conditions, algorithm transparency (how does it handle artifact?), and uptime/serviceability. Also check integration ease: will the monitor export CTG files to your EMR without manual steps? I recommend short pilot runs on actual floors, not demos — 30 consecutive births over four weeks is a practical sample. Try it; you’ll spot patterns fast. — three quick metrics to evaluate vendors: signal fidelity under motion, false alarm rate in live trials, and maintenance turnaround time. I’ve shared these lessons with procurement teams across Asia and Europe, and when systems meet those checks they actually reduce interventions. Trust me — the right data will calm teams and protect moms. COMEN
